

Happy Birthday, Mark!
June 5, 2023
1st Day of Intern Orientation
June 19, 2023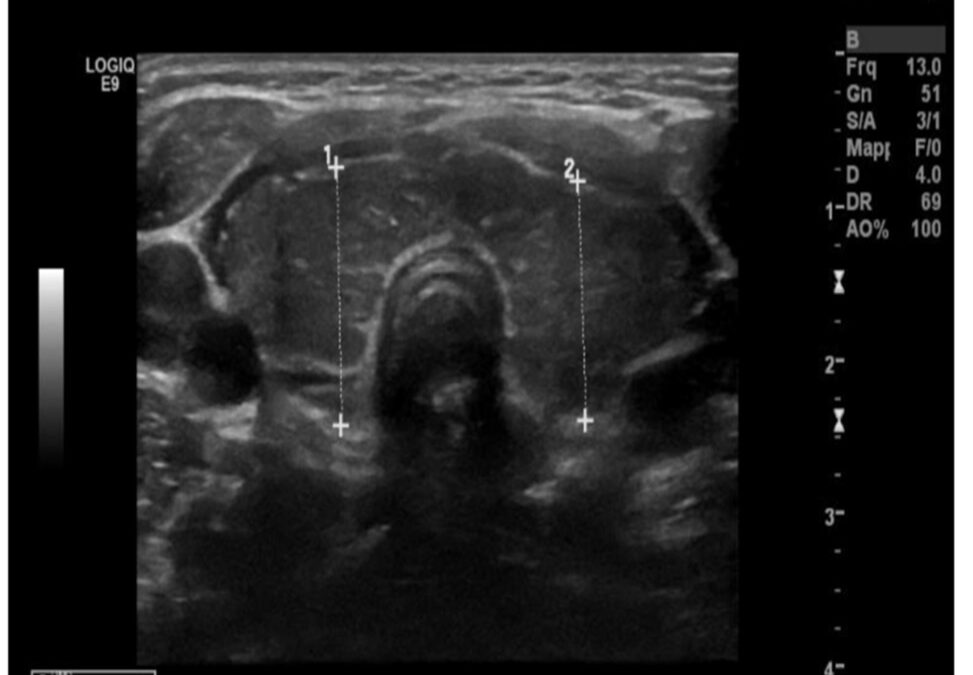
This is the slogan
The following is a case report published by our upcoming PGY-3 Dan Kallush, detailing a medical phenomenon called Periodic paralysis, which in this case was occurring in a pediatric patient.
Author’s Name: Daniel Kallush
Department:Emergency Dept
Email Address:Daniel.kallush@crozer.org
Abstract Category: Case Report
Title: A Case of Thyrotoxic Periodic Paralysis
Authors:Dr. Daniel Kallush, PGY-2 DO
Periodic paralysis (PP) is a muscle disease in the family of diseases called channelopathies, manifested by episodes of painless muscle weakness. PP is classified as hypokalemic when episodes occur in association with low potassium blood levels or as hyperkalemic when episodes can be induced by elevated potassium. Most cases of PP are hereditary, usually with an autosomal dominant inheritance pattern. Thyrotoxic PP has been most widely reported and studied in East Asian populations, in which the incidence among patients with hyperthyroidism is approximately 2 percent. Hypokalemic thyrotoxic hypokalemic periodic paralysis is a condition characterized by a triad of acute hypokalemia without total body potassium deficit, episodic muscle paralysis, and thyrotoxicosis.
We present a case of a Latino male, 15 years of age with bilateral muscle weakness, hypokalemia, and QTc prolongation on serial EKGs who was subsequently found to have new onset hyperthyroidism and longstanding Graves’ Disease.
Background/Objective:
Hypokalemic thyrotoxic hypokalemic periodic paralysis is a condition characterized by a triad of acute hypokalemia without total body potassium deficit, episodic muscle paralysis, and thyrotoxicosis. Although thyrotoxicosis affects females nine times more frequently than males, TPP occurs more commonly in men (male to female ratio ranging from 17:1 to 70:1)[1], and it occurs in higher rates in males of Asian and Polynesian descent. The prevalence in North America is 0.1%–0.2%, but the incidence is expected to rise in the future in both Europe and North America due to immigration patterns.
The pathophysiology though poorly understood is considered to be due to the thyroid hormone stimulation of the sodium-potassium-adenosine triphosphatase pump resulting in in an intracellular potassium shift and resulting serum hypokalemia without total body potassium deficits. The association with the presence of HLA-DRW8 suggests that the basic defect may be genetically determined, but the precise pathology of TPP is mainly through Na+-K+-ATPase pump[2]. The presence of excessive thyroid hormone in serum seems necessary for this disorder. Thyroid hormone, β-adrenergic catecholamine, and insulin can increase the Na+-K+-ATPase pump activity in skeletal muscles, liver, and kidneys. Given that total body potassium is not truly depleted this may explain why weakness resolves when potassium returns to the extracellular space. Derangements in calcium, magnesium, and phosphate may also be attributable to causes of muscular weakness. Male sex hormones tend to increase Na+/K+-ATPase activity, which is a tentative explanation as to why males are at a higher risk of TPP despite autoimmune disease and thyroid diseases generally being more common in the female population. An increased Na+/K+-ATPase activity leads to shifting of potassium into the cells. In other types of potassium derangements, the acid-base balance is usually disturbed, with metabolic alkalosis and metabolic acidosis often being present. In TPP, these disturbances are generally absent. Low potassium levels in the serum lead to hyperpolarization of skeletal muscle cells, making the neuromuscular junction less responsive to normal nerve impulses, which in turn decreases the contractility of the muscles.
While patients with thyrotoxic PP do not have the genetic mutations associated with familial hypokalemic PP, it has been suggested that individuals who are susceptible to thyrotoxic PP may have an ion channel defect, which, in the euthyroid state, is not sufficient to produce symptoms. A number of studies have identified specific susceptibility loci that confer risk for thyrotoxic PP. Many but not all of these affect KCNJ2 expression; this gene encodes Kir2.6, an inwardly rectifying potassium channel, expressed in skeletal muscle that is transcriptionally regulated by thyroid hormone. Some but not all of these loci have been implicated in Graves’ disease. The frequency of these genes varies in different ethnic populations, which is thought to explain the higher prevalence of thyrotoxic PP in these populations[3].
Thyrotoxicosis can be associated with TTP, however Graves disease is the most common. Often the illness may or may not present with the usual symptoms of hyperthyroidism but nonetheless prompt recognition is needed for appropriate management. Attacks vary in frequency and duration [9, 15]. Duration of symptoms of several hours is typical, but can range from minutes to days. As with hypokalemic PP, any events that are associated with an increased release of epinephrine or insulin can precipitate TPP, causing movement of potassium into cells and low potassium blood levels [9, 16]. Most commonly, the inciting event is either rest after strenuous physical activity, stress, or a high-carbohydrate load. Other events reported to induce attacks in TPP include cold exposure, infection, alcohol intake, pulse corticosteroid therapy, and menses [9, 12, 17]. In many instances, no obvious precipitant is identified.
Results (Case description):
A 15 year old Latino male with no significant medical history presented to an emergency department with complaints of bilateral lower extremity paralysis and being unable to walk. The patient reports having a similar episode approximately one year ago that was transient and that spontaneously resolved without need for hospitalization. Patient reports being in his usual state of health until he went to an all you can eat buffet with his family the prior night and woke up at 4 AM the following morning with nausea vomiting and being unable to ambulate. Patient further reported having profound weakness in both of his legs. He was unable to ambulate to the bathroom and when he called for his parents they called 911. He denies any trauma. He denies any use of drugs, alcohol, diuretics, laxatives, or anabolic sports supplements. There is no family history of such a condition.
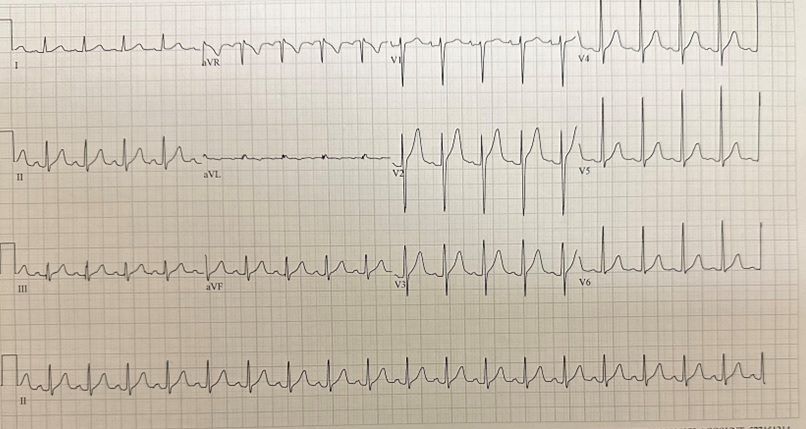
Presenting vital signs showed an afebrile (98.2), tachycardic (HR-130), normotensive (121/85), and non hypoxic (99% on RA) male. Physical exam was notable for anxious appearing male with a normocephalic atraumatic head with no meningismus PERRLA CTA bilaterally and tachycardic with 5/5 strength in his upper extremities with motor and sensation grossly intact and 2/5 strength in his lower extremities with motor and sensation grossly intact. Normal reflex intact throughout. Initial laboratory evaluation showed a potassium of 1.3 with no other electrolyte abnormalities. No leukocytosis. Elevated troponin of 115 and a CK of 445. Initial EKG showed sinus tachycardia with a QTc of 616.
Patient was started on supplemental potassium with a 20 mEq K rider parenterally and was transferred to a PICU for further level of care. Repeat ECG with transport showed a sinus tachycardia at 121 BPM with a QTc of 541. On arrival to the PICU patient had repeat laboratory testing and ECG completed showing a potassium of 4.5 and a QTc of 445. Downtrending troponins and CK. Noted to have decreased Calcium and elevated phosphate.
Noted new electrolyte derangements prompted further investigation. Thyroid and parathyroid studies were ordered and found to be 0.02, total T3 of 412, and a T4 level of 24.5. Prompting further evaluation endocrinology was consulted and a thyroid ultrasound was ordered.
Endocrinology evaluated the patient with recommendation for adding thyroid autoantibodies t the patient work up. Initiating Methimazole 20 mg BID and daily CMP with rechecking thyroid studies in two weeks time. Ultrasound of the thyroid revealed bilateral lobe enlargement with echogenicity and increased vascularity compatible with thyroiditis.
Patient was found to have new onset hyperthyroidism with thyroglobulin antibodies elevated at 7 along with elevated thyroid peroxidase antibodies at 374. Diagnosis of hypokalemic periodic paralysis secondary to longstanding Graves disease was confirmed. Patient was stabilized with complete resolution of symptoms and transferred to a general medical floor with endocrinology remaining on board for consultation and soon after discharged with appropriate education and familial instruction and outpatient follow up with endocrinology.
Conclusion:
Given the repeat nature of the patient’s symptoms and findings of reported chronic tremor patient likely had longstanding Graves’s disease that became manifest with this episode of periodic thyrotoxic paralysis. Periodic paralysis is an uncommon presentation of Graves’ disease and is associated with electrolyte abnormalities such as severe hypokalemia. While its epidemiology is observed most in those of eastern Asian descent it is possible to be witness in any group. Patients that present with this pattern of disease are typically asymptomatic until some type of clinical stressor aggravates their underlying susceptibility and causes severe muscle weakness and paralysis.
Due to the rarity of the condition awareness should be raised and suspicions heightened in the setting of by a triad of acute hypokalemia without total body potassium deficit, episodic muscle paralysis, and thyrotoxicosis. Physicians should keep TPP on their differential in adolescent patient presenting with lower extremity paralysis and hypokalemia. Extensive history details and comprehensive physical exam with appropriate laboratory evaluation of electrolyte and hormone levels should be used for prompt diagnosis.
References (Minimum of three references within the last 10 years):
Bibliography
1. UpToDate. www.uptodate.com. Accessed March 6, 2023. https://www.uptodate.com/contents/thyrotoxic-periodic-paralysis?search=thyrotoxic%20periodic%20paralysis&source=search_result&selectedTitle=1~15&usage_type=default&display_rank=1
2. Patel M, Ladak K. Thyrotoxic Periodic Paralysis: A Case Report and Literature Review. Clinical Medicine & Research. 2021;19(3):148-151. doi:https://doi.org/10.3121/cmr.2021.1610
3. Munir MD I, Mehmood MD T, Islam K, Soni L, I. McFarlane S. Thyrotoxic Periodic Paralysis with Sensory Deficits in Young African American Male: A Case Report and Literature Review. American Journal of Medical Case Reports. 2020;7(7):138-142. doi:https://doi.org/10.12691/ajmcr-7-7-5
4. Tella SH, Kommalapati A. Thyrotoxic Periodic Paralysis: An Underdiagnosed and Underrecognized Condition. Cureus. Published online October 6, 2015. doi:https://doi.org/10.7759/cureus.342
5. Jung SY, Song KC, Shin JI, Chae HW, Kim HS, Kwon AR. A case of thyrotoxic periodic paralysis as initial manifestation of Graves’ disease in a 16-year-old Korean adolescent. Annals of Pediatric Endocrinology & Metabolism. 2014;19(3):169. doi:https://doi.org/10.6065/apem.2014.19.3.169


{kind=link}
{kind=link}
{kind=link}