
In-Person Conference!
May 5, 2021
Congratulations to Raghav on publishing a case
May 27, 2021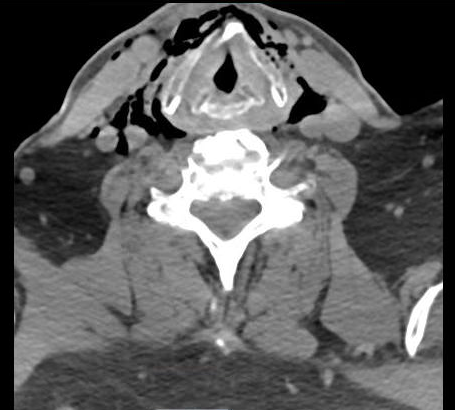
HPI: 63 year old male presented to the Emergency Department for traumatic anterior neck injury after slipping in the bathroom and striking his neck directly on the sink counter.
ROS: Patient complained of hoarse voice, difficulty swallowing, and blood-tinged sputum.
Physical Exam: Vitals stable, saturating well on room air, airway intact, no acute distress, anterior neck crepitus.
Labs: Patient was incidentally found to be COVID positive.
CT imaging: right thyroid cartilage and hyoid bone fracture, soft tissue emphysema in neck and mediastinum and traumatic laryngeal rupture.
NPL: right-sided hematoma and airway swelling.
ED Course: Patient was placed in isolation due to positive COVID result. Early CT scans and trauma surgery consults were obtained due to stable nature, history and physical. NPL was performed with ENT at bedside. Trauma surgery recommended close monitoring in the hospital. ENT recommended steroids to decrease airway inflammation and airway monitoring. Infectious disease agreed with plan to cover with cefepime, doxycycline, metronidazole, fluconazole. Cardiothoracic surgery recommended continued monitoring and no surgical intervention for mediastinitis at the time. The patient’s condition remained stable throughout his stay in the ED. Patient was admitted to Step-Down Unit.
CT neck w/o contrast:
1. Fractures of the right thyroid cartilage and hyoid bone.
2. Large amount of soft tissue emphysema in the neck, involving the retropharyngeal space and bilateral deep soft tissues. There is abnormal contour of the right side of the supraglottic laryngeal airway as well as laryngeal mucosal edema. Findings are therefore suspicious for laryngeal injury/traumatic laryngeal rupture.
—
Summary:
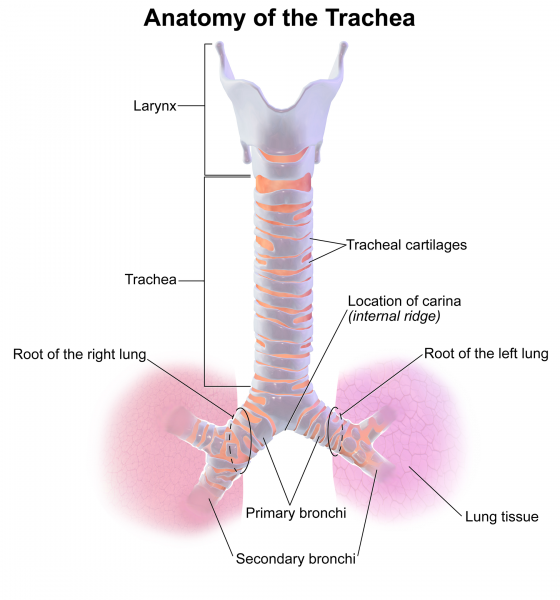
This patient sustained a laryngeal injury from a direct strike to the neck from the edge of the sink counter. This mechanism is often described as a “clothes-line” injury but can also be from a penetrating injury, and strangulation. Priority lies in airway management with EARLY specialist consultations (ENT, trauma surgery, anesthesia). Laryngoscopy can be used to visualize the extent of the damage. If indicated, the preferred method of airway control is an awake fiberoptic oral intubation. As always, be prepared for an emergent surgical airway.
—
References
- https://wikem.org/wiki/Tracheal_injury
- Rosen’s Emergency Medicine – Concepts and Clinical Practice
{kind=link}
{kind=link}