
Crozer Crew gets Vaccinated!
December 23, 2020
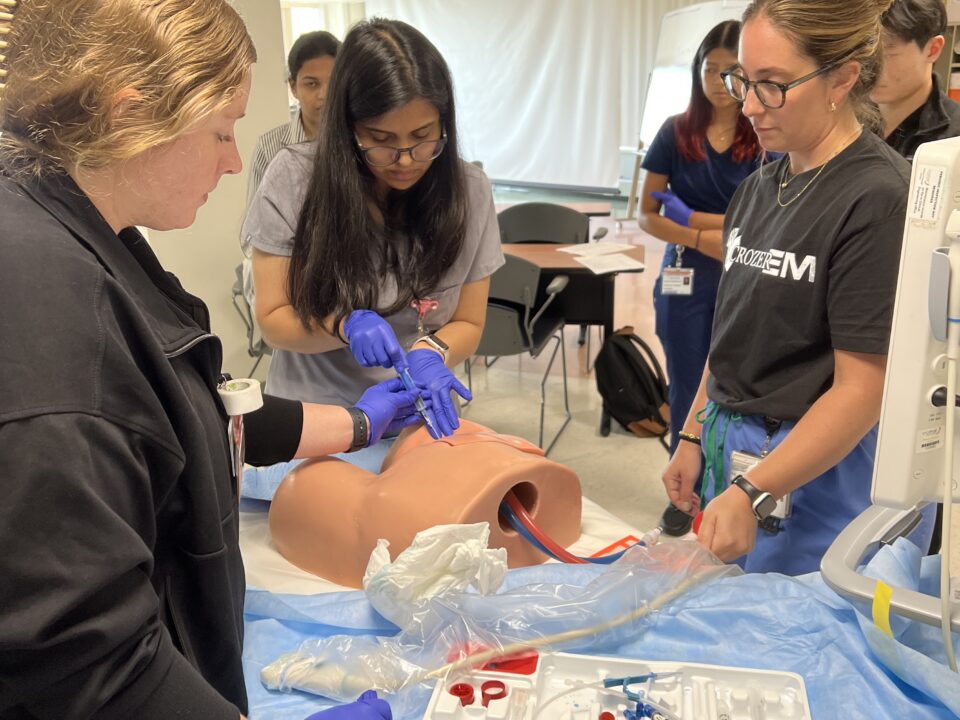
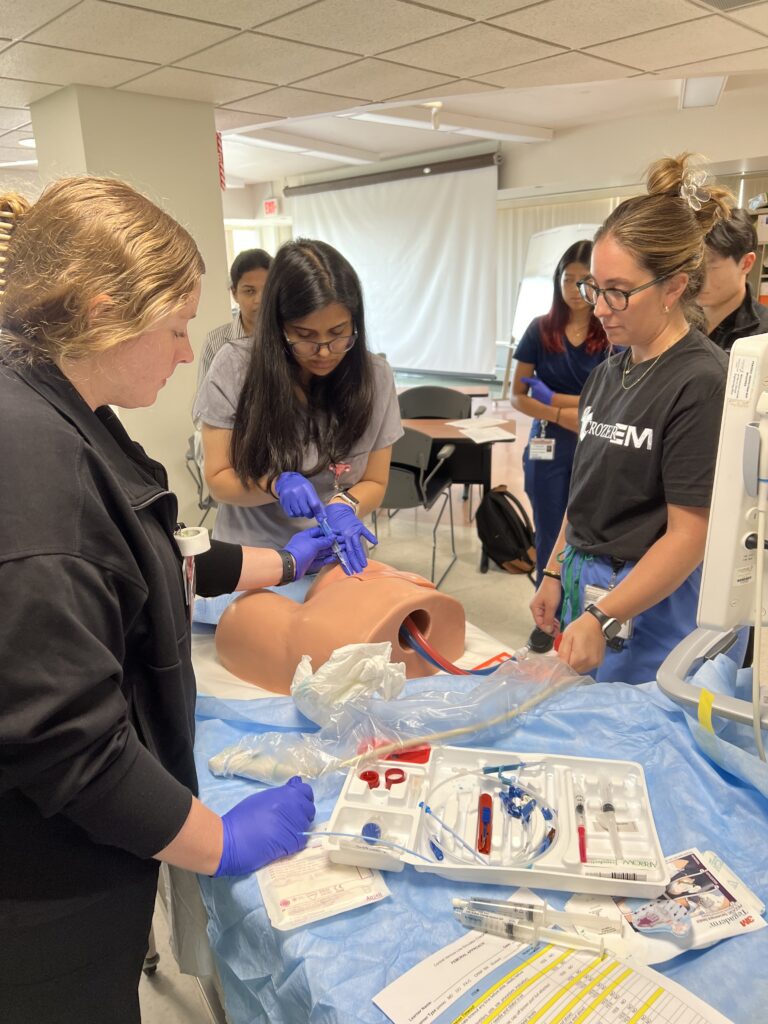
Ultrasound-Guided Central Line Workshop
April 5, 2021By: Karima Sajadi, MD and Wajid Ali, MD
HPI:
40 year old male with a history of polysubstance abuse presented to the ED complaining of intesnse pain and swelling in his right lower extremity (RLE) for the past 2 days. Patient used heroin two consecutive nights in a row prior to presentation and presents falling asleep with his RLE folded underneath his body. When he woke up in the morning, the leg was swollen and painful to touch. Patient states he could not move his leg due to severe pain. As the day progressed, the patient noticed increasing pain and swelling of the leg in addition to the leg turning a blue-ish color. The patient then presented to the ED.
Upon arrival in the ED, the patient was hypotensive, tachycardic, complaining of severe pain in his RLE.
Physical Exam:
The knee was severely tender to touch and the soft tissue was extremely tense. Appearance of the RLE is shown below:

Labs:
WBC 18.4, Hgb 8.0
Na 133, K 6.2, Ca 6.0, Cr 6.4, GFR 10
Lactate 10
CK 188
With this history, compartment syndrome was strongly suspected. Compartment pressures were measured with a Stryker device. Compartment pressures of the RLE were as follows:
Anterior compartment: 19 mmHg
Lateral compartment: 16 mmHg
Posterior compartment: 4 mmHg
IV fluid resuscitation and broad-spectrum IV antibiotics were initiated. Surgery was consulted and the patient was taken to the OR emergently for fasciotomy.
Compartment Syndrome
Consider compartment syndrome after:
- fracture (most common)
- crush injury
- immobilization
- snake bites, burns
- prolonged tourniquet application
- fluid extravasation into a limb
- soft tissue infection
- extreme exertion
Immediate threats: nerve and muscle viability
Later threats: infection, gangrene, rhabdomyolysis, renal failure
Clinical Symptoms:
- Compartment is swollen, tender, firm
- Usually apparent after trauma/injury, but may be delayed up to 48 hours after the event
- The 5 P’s:
- Pain (early)
- Paresthesia (early)
- Pallor
- Paralysis (late)
- Pulselessness (late)

Workup:
- X-ray to evaluate for fracture
- Compartment pressure measurements (Stryker device)
- normal is <10 mmHg
- Delta Pressure:
- Delta pressure = Diastolic BP – Compartment pressure
- Delta pressure < 30 mmHg is suggestive of compartment syndrome
- Total CK to evaluate for rhabdomyolysis
- Chemistry for hyperkalemia/renal failure
Management:
- ABC’s
- IV fluid resuscitation
- Antibiotics
- Analgesia
- Supportive treatment for rhabdomyolysis, renal failure, hyperkalemia, etc.
- Emergent OR for fasciotomy
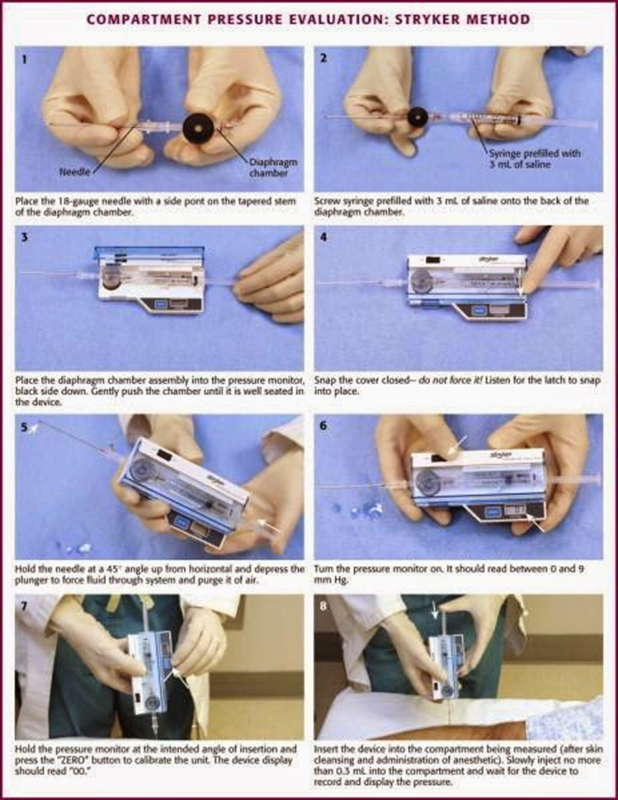
Stryker Device
The Stryker device is a type of hand-held manometer which performs direct measurements of compartment pressures.
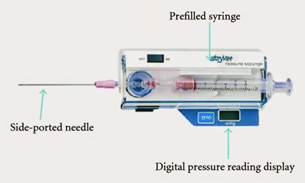
This is a great diagram from emcurious.com:
References:
- https://wikem.org/wiki/Compartment_syndrome
- http://www.emcurious.com/blog-1/2014/12/11/compartment-pressure-measurement-stryker-it
{kind=link}
{kind=link}